How is it possible that people are still dying for lack of oxygen in 2026?

70%
“70% of people in Low-and-Middle-Income-Countries (LMICs) don’t have access to medical oxygen.”
Lancet Global Health Commission on medical oxygen security (2025)
91%
“In Sub-Saharan Africa, it’s even worse. 91% of people who need oxygen for acute medical or surgical care do not receive it.”
Lancet Global Health Commission on medical oxygen security (2025)
70%
“70% of people in Low-and-Middle-Income Countries (LMICs) don’t have
access to medical oxygen.”
Lancet Global Health Commission on medical oxygen security (2025)
91%
“In Sub-Saharan Africa, it’s even worse. 91% of people who need oxygen for acute medical or surgical care do not receive it.”
Lancet Global Health Commission on medical oxygen security (2025)
Didn’t we solve this during COVID already?
Over the last decade, billions of dollars were invested to try and solve the oxygen crisis.
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
A lot of the money that flowed into Sub-Saharan Africa bought one-off equipment purchases.
In Nigeria alone, more than 100 oxygen production plants were built.
Over the last decade, billions of dollars were invested to try and solve
the oxygen crisis.
2015
2016
2017
2018
2019
2020
2021
2022
2023
2024
2025
2026
A lot of the money that flowed into Sub-Saharan Africa bought one-off equipment purchases.

In Nigeria alone, more than 100 oxygen production plants were built.
But just because the equipment is there, doesn't mean patients are able to access oxygen.

To connect oxygen to
patients who need it requires
a network of people
and services.
Local businesses that maintain equipment, manage last-mile delivery, train staff, and guarantee supply.
And that network needs the right conditions to grow and thrive.
One that provides regulations,
tariffs, and access to capital.
To connect oxygen to patients who need it
requires a network of people and services.
Local businesses that maintain equipment, manage last-mile delivery, train staff, and guarantee supply.
And that network needs the right conditions to grow and thrive. One that provides regulations, tariffs, and access to capital.

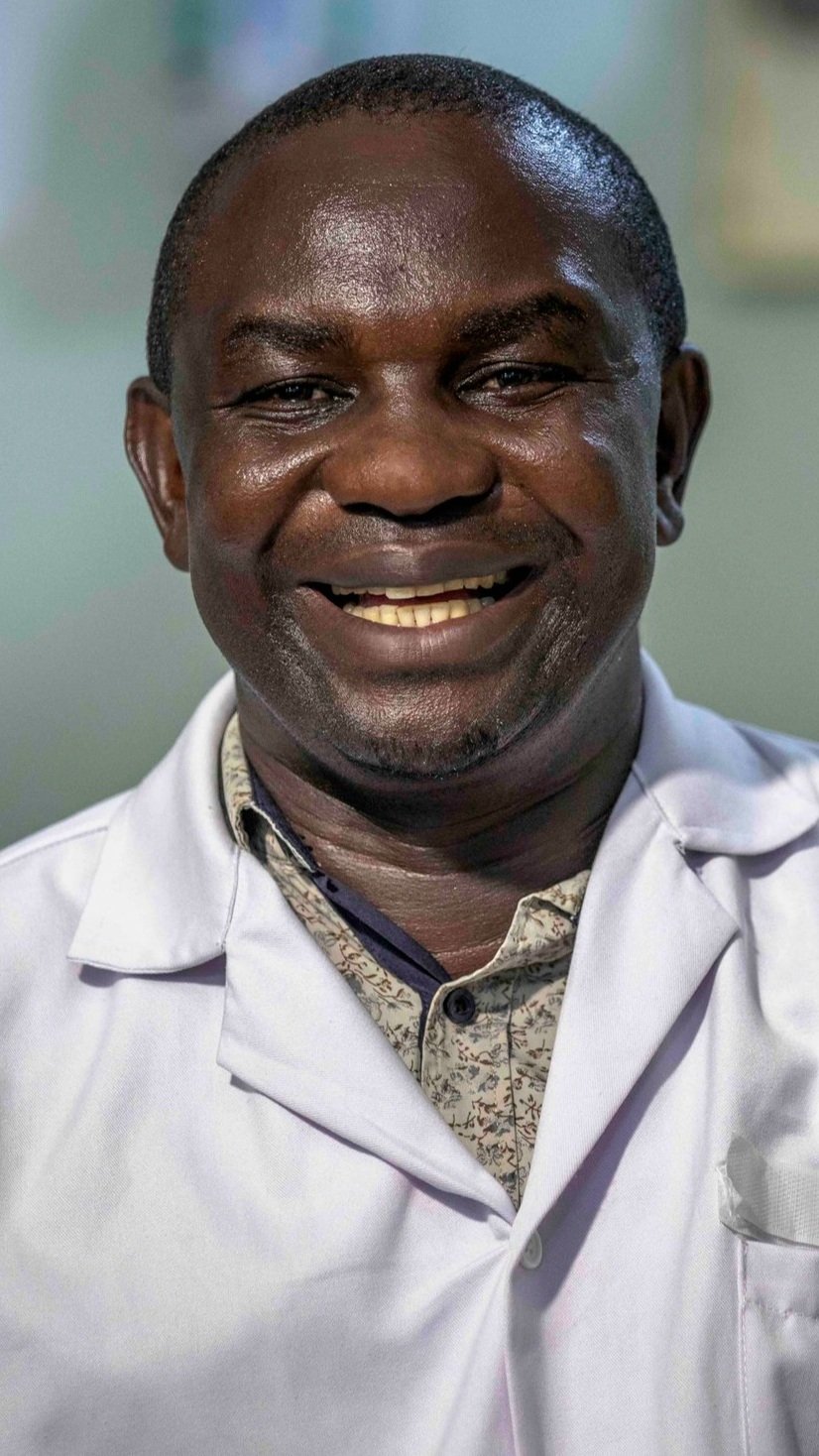
“When concentrators break or cylinder deliveries are irregular, patients go without oxygen. And that’s when deaths rise.”
Dr Birungi Julius, Acting Medical Superintedent,
Kagadi, Uganda.

“When concentrators break or cylinder deliveries are irregular, patients go without oxygen. And that’s when deaths rise.”
Dr Birungi Julius, Acting Medical Superintedent, Kagadi, Uganda.

“My sister gave birth to premature twins. They were put on oxygen, but two days later, the oxygen ran out, and we lost them both.”
Hilda Bugingo, FREO2 Project Engineer.

“My sister gave birth to premature twins. They were put on oxygen, but two days later, the oxygen ran out, and we lost them both.”
Hilda Bugingo, FREO2 Project Engineer.
In a post-aid era, with shrinking health budgets, we can’t
keep buying equipment and assuming the job is done.
This isn't just an oxygen problem. 40% of medical equipment in LMICs is typically out of service.
We need to build systems that ensure patients have access to
reliable health services beyond funding cycles.
This isn't just an oxygen problem.
40% of medical equipment
in LMICs is typically out of service.
In a post-aid era, with shrinking health budgets, we can’t keep buying equipment
and assuming the job is done.
We need to build systems that ensure patients have access to reliable health services beyond funding cycles.
We've already proven that this can be done for medical oxygen
Over the last half decade, we’ve been working with local respiratory care businesses in Nigeria, Uganda, Tanzania, and Kenya, who provide 24/7 access to oxygen for patients who need it.
For an agreed recurring fee they get the oxygen to where it needs to be, taking responsibility for managing oxygen stock levels, equipment uptime, maintenance and training, so that hospitals can focus on patient care.
In Nigeria, HealthPort’s partner hospitals once met just 10% of their oxygen demand. Now, they have oxygen available 100% of the time.
What’s more, by improving supply reliability alone, HealthPort have seen oxygen use increase by 50-70%.
In Uganda, FREO2 recorded that oxygen was running 100% of the time despite 215 power outages over a three month period.
In Kenya, CPHD have shown that reliable oxygen access can be delivered at less than KES 200/$1.55 per capita per year. This is comparable to the cost of routine vaccines.



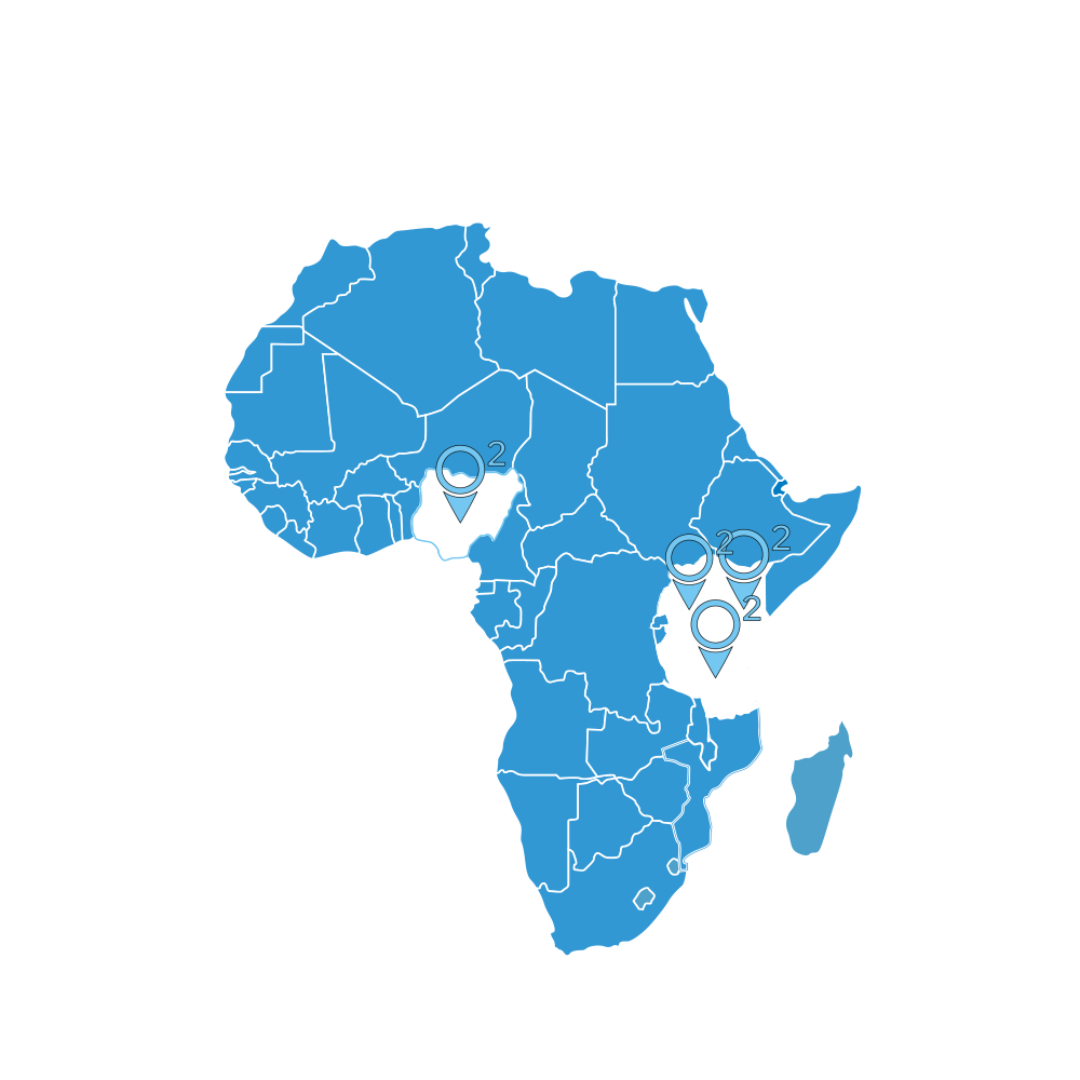
Over the last half decade, we’ve been working with local respiratory care businesses in Nigeria, Uganda, Tanzania, and Kenya, who provide 24/7 access to oxygen for patients who need it.
For an agreed recurring fee they get the oxygen to where it needs to be, taking responsibility for managing oxygen stock levels, equipment uptime, maintenance and training, so that hospitals can focus on patient care.
Nigeria
In Nigeria, HealthPort’s partner hospitals once met just 10% of their oxygen demand. Now, they have oxygen available 100% of the time.
What’s more, by improving supply reliability alone, HealthPort have seen oxygen
use increase by 50-70%.

Uganda
In Uganda, FREO2 recorded that oxygen was running 100% of the time despite 215 power outages over a three month period.

Kenya
In Kenya, CPHD have shown that reliable oxygen access can be delivered at less than KES 200/$1.55 per capita per year. This is comparable to the cost of routine vaccines.

“As a hospital manager, I have many many issues every day. Since HealthPort got here, oxygen is not one of them!”
Folasade Fadare, Harvey Road Hospital, Yaba, Lagos, Nigeria.
“As a hospital manager, I have many many issues every day. Since HealthPort got here, oxygen is not one of them!”
Folasade Fadare, Harvey Road Hospital,
Yaba, Lagos, Nigeria.
What’s needed to close the
oxygen access gap across
Sub-Saharan Africa?
What’s needed to close the oxygen access gap across
Sub-Saharan Africa?

We need to invest in local respiratory care businesses who are running the networks of people and services needed to keep oxygen flowing.
Not only will we prevent up to
800,000 child deaths each year.
But we’ll demonstrate what it looks like to move from aid to investment in the face of shrinking budgets.
We need to invest in local respiratory care businesses who are running the networks of people and services needed to keep oxygen flowing.
Not only will we prevent up to
800,000 child deaths each year.
But we’ll demonstrate what it looks like to
move from aid to investment in the face
of shrinking budgets.
Fund
what lasts
Back local respiratory
care businesses
We’re inviting progressive funders to back the teams keeping oxygen available day and night. Fund them with the right kind of capital and support to grow.
Fund their operating environment
Fund the “boring but decisive” conditions:
fit-for-purpose regulation and tariffs, smarter procurement, and processes that make smaller investments feasible.
Unlock
what's next

Every hospital needs oxygen but it’s one of the hardest essential services to keep running 24/7. Prove this model in respiratory care, and you have a template for other lifesaving services.
Fund
what lasts
Back local respiratory
care businesses
We’re inviting progressive funders to back the teams keeping oxygen available day and night. Fund them with the right kind of capital and support to grow.
Fund their operating environment
Fund the “boring but decisive” conditions:
fit-for-purpose regulation and tariffs, smarter procurement, and processes that make smaller investments feasible.
Unlock
what's next
Every hospital needs oxygen but it’s one of the hardest essential services to keep running 24/7. Prove this model in respiratory care, and you have a template for other lifesaving services.
The funding landscape is shifting from aid to investment. In 2026 the question isn't whether to change, but how. If you want to make the shift real, fund what lasts: local businesses and the conditions that let them deliver reliably long after the grant cycle ends.
Learn More
The funding landscape is shifting from aid to investment. In 2026 the question isn't whether to change, but how. If you want to make the shift real, fund what lasts: local businesses and the conditions that let them deliver reliably long after the grant cycle ends.