
Building a resilient oxygen market in Uganda
A map of supply and demand
In COVID-19, like many countries, Uganda received significant investment into oxygen production. However, this hasn’t led to all patients having access to oxygen when they need it. What’s more, the size, shape and nature of the medical oxygen market has remained unknown, making it hard to make positive adjustments.
In March 2026, the Oxygen CoLab undertook a series of engagements with oxygen players across Uganda, in order to create greater visibility of the current oxygen market, and inform decisions that can shape the market towards a state of much greater oxygen access for all.

Who did we engage?
26
Manufacturers
PSA plant operators, industrial & hospital-based producers
2
Regulatory actors
National Drug Authority (NDA) & District Health Officers
52
Distributors
Wholesalers, regional specialists, industrial SMEs, micro-distributors
2
Trade Associations
Uganda Manufacturers Assoc. (UMA) & Uganda Healthcare Federation (UHF)
188
Health Facilities
Private not-for-profit , private, government in Central, Eastern, Western, and Northern
4
Development Orgs
International and local organisations supporting oxygen access
If you are working on improving access to oxygen in Uganda, these insights are for you.
Uganda’s oxygen challenge is no longer a supply problem. It’s a connection problem.

In Uganda, true unmet oxygen need is considerably higher than purchasing data suggests
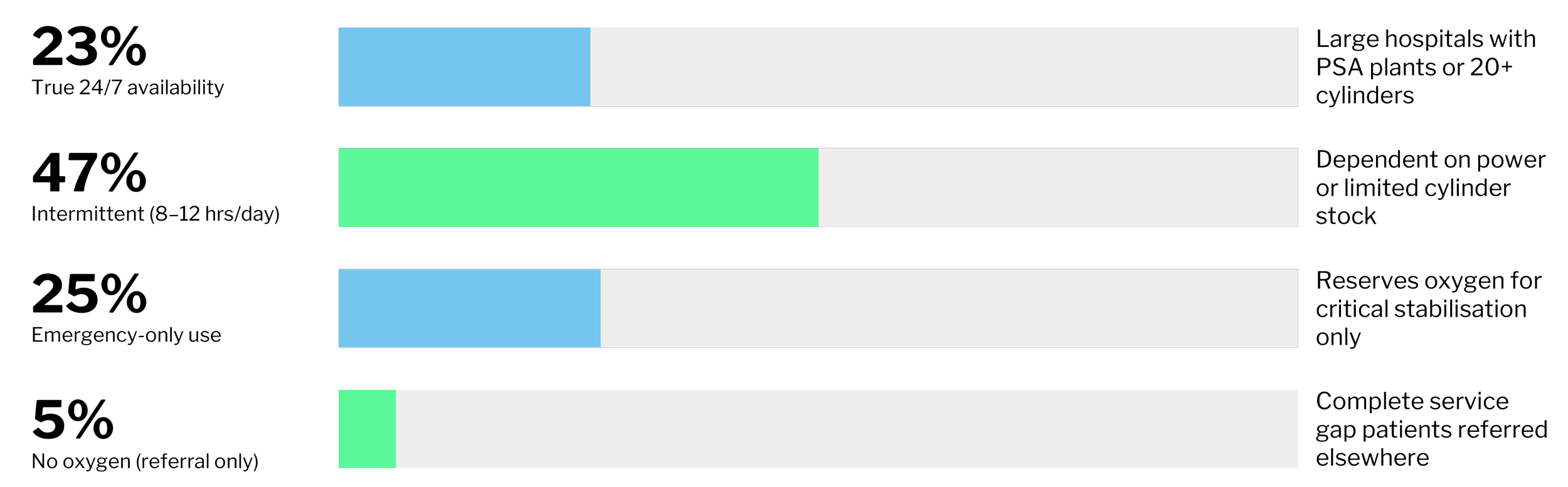
Along with prohibitively high costs, nearly half of private and private not-for-profit facilities (PNFPs) report significant delivery delays, and 23% have experienced stock-outs with no alternative source available. Such experiences have led facilities to struggle trusting the reliability of medical oxygen supply, leading to rationing behaviours such as referring patient cases that require a lot of medical oxygen to other health facilities, or reserving oxygen for only the most critical cases, rather than all clinically indicated patients.
The production is present
Twenty-six private manufacturers operate PSA plants across all four regions, with a combined weekly output of 4,200–7,300 cylinders at a 76% plant utilisation rate. This exceeds the estimated national medical demand of 3,000–4,000 cylinders weekly.
The market has three distinct layers, all present across Uganda’s regions ↓
-
Produce oxygen primarily for their own cutting and welding operations. They sell surplus commercially, 75% of which is to industrial customers.
Medical oxygen is a secondary by-product rather than a core business driver, meaning quality assurance and healthcare facility relationships receive little attention and no delivery or support services.
-
Produce medical oxygen through on-site PSA plants and sell limited surplus to Private-not-for-Profit (PNFP) and private hospitals within a 50km catchment area.
They represent only 5% of market share, yet are disproportionately significant in underserved regions. Just two facilities alone meet the demand of 80% of private health facilities in the Northern and far Eastern regions.
-
Purpose-built oxygen businesses dedicated to gas production and distribution. 60% of their customer base is medical facilities and national distribution networks.
Two dominant players supply 58% of surveyed health facilities nationwide. The rest of the market largely fails to replicate the standard of their medical-grade oxygen quality and comprehensive service models.

Geographical divide creates inequality of supply
46% of facilities report significant delivery delays and 23% have been left with no alternative when their supplier is out of stock.
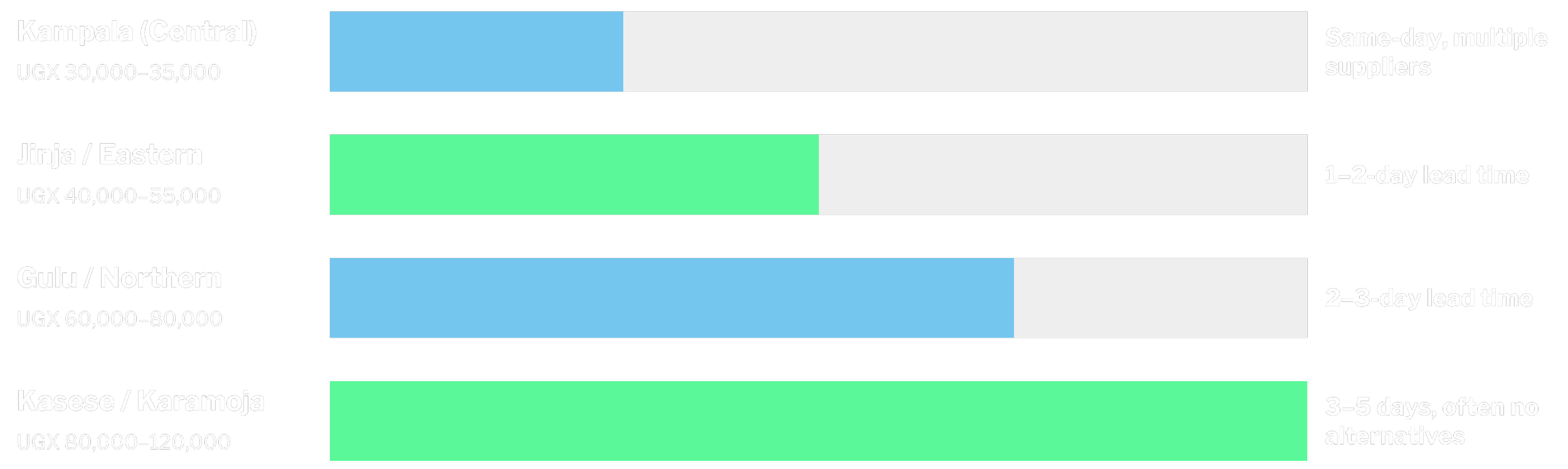
How far oxygen needs to travel to reach a facility matters. 80% of production capacity is within 100km of Kampala-Jinja and 15 districts have two or fewer suppliers, with areas like Moroto requiring journeys of 200–400 km to access oxygen.
Transport costs represent 40–60% of the final price in remote areas. The UGX 20,000–50,000 cost per cylinder is driving a geographic premium that market forces alone will not fix.
However, there are models showing promise. Producers in the Northern Region serve 80% of private health facilities within a 50km radius, providing a proof-of-concept for decentralised regional production that could address geographic gaps.
Regulation does not serve oxygen access
The backbone of the oxygen supply system is not formal supply chains, but a network of small, informal distributors, garages, hardware shops, and traders operating oxygen as a side business.
Most manage just 2–15 cylinders, with no dedicated vehicles, no buffer stock, and limited medical oversight.
Medical oxygen is regulated as a pharmaceutical product in Uganda, under NDA oversight. However processes for complying to national regulation are unclear, slow, and expensive for most suppliers.
of distributors lack NDA medical oxygen certification.
91%
of customer facilities reported receiving half filled cylinders while being charged full price.
33%
of manufacturers report standard Good Manufacturing Practice training.
83%
years, the longest reported timeline for receiving NDA approval.
2+
of distributors operate with no certifications whatsoever.
27%
of all oxygen sector actors do not belong to any trade association, limiting advocacy and collective dialogue.
72%
The evidence from this mapping is clear: Uganda’s oxygen gap is now shaped less by national supply and more by weak market connections between producers, distributors, and facilities. Building a resilient oxygen market will require targeted action on distribution, regulation, and regional market development.
Oxygen CoLab is working to build resilient local oxygen markets by tackling the barriers that stop supply from reaching patients: fragmented procurement, unclear regulation, under-supported SMEs, and invisible financing. Across these four areas, we are helping governments and suppliers create the conditions for reliable, investable oxygen services that can last beyond grant funding.
This report was prepared by Dorcas Kemigisha and OLK HealthTech Consults.